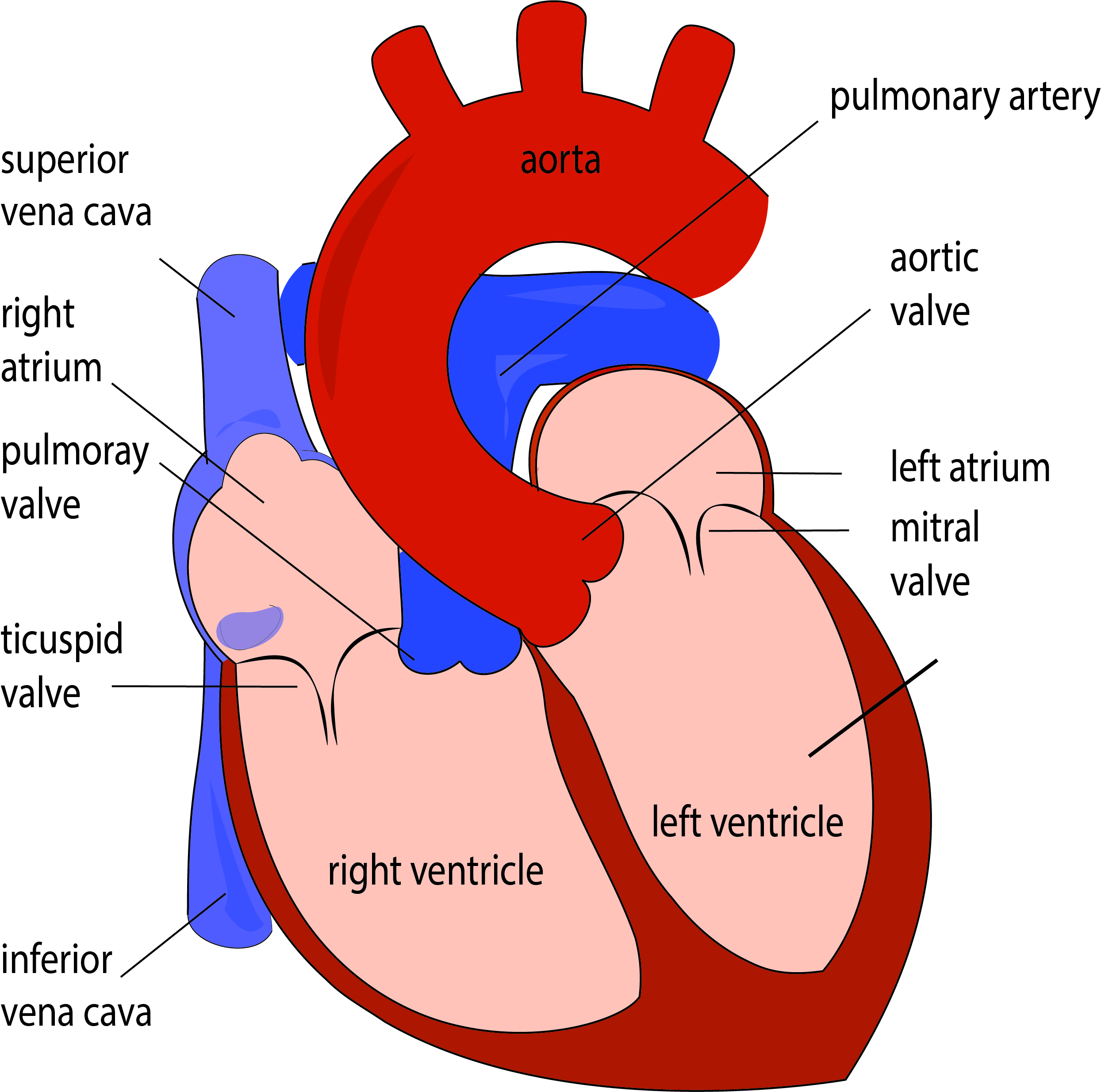
The heart is located behind the chest bone and slightly displaced to the left side. It is a hollow muscular organ that is pumping the blood throughout our body. The heart consists of two atria and two ventricles. Four heart valves alternatively open and closes during the heart cycle, providing the unilateral blood through the heart chambers. The tricuspid valve is positioned between the right atrium and the ventricle while the pulmonary valve is located between the right ventricle and the pulmonary artery. Those valves are located on the right side of the heart, pumping the venous blood to be oxygenated in the lungs. The left heart side is pumping oxygen-rich blood that is coming from lungs throughout our body. The Mitral valve is located between the left atrium and ventricle, while the aortic valve is between the heart and the aorta.
HUMAN HEART ANATOMY AND PHYSIOLOGY
The heart cycle consists of alternate contractions and relaxations, known as systole and diastole. The average human heart beats 60 – 100 beats per minute, and ejects around 70 ml of blood with each contraction, making 5 liters of blood pumped every minute in the average person of 75 kg. The blood is ejected into the aorta, the biggest arterial blood vessel in a human body. Aortic branches, after that, provide blood delivery to the head, limbs, and organs. Coronary arteries, the first aortic branches, perfuse the heart.
ANGINA PECTORIS
Angina pectoris is a symptom of coronary arteries stenosis. Atherosclerosis obstructs the arteries by cholesterol plaques that are reducing the blood delivery to the myocardium. During the physical activity, insufficient oxygen delivery to the myocardium results in chest angina pain, which eventually subsides during the rest. The pain could spread up to the jaw or down the arm. That is stable angina pectoris. In advanced disease, chest pain will appear even during the rest. Now we are talking about unstable angina. If untreated unstable angina eventually results in myocardial infarction.

MYOCARDIAL INFARCTION
Myocardial infarction is a permanent heart muscle damage. It could develop suddenly, due to coronary arteries thrombosis or gradually during the chest angina. Patients with myocardial infarction experience excruciating chest pain, sweating and fall in blood pressure, frequently followed by arrhythmias. If severe, infarction could result in a shock and sometimes death.
Myocardial damage is permanent, and symptoms in those who survive to depend on the infarction extent. Reduced physical activity, arrhythmias, heart failure, and mitral valve insufficiency are some severe complications.
ATHEROSCLEROSIS PREVENTION
High blood pressure, diabetes, high blood cholesterol, smoking, and positive family history are the major risk factors for atherosclerosis and coronary artery disease. Medications could stop atherosclerosis development to some degree, but without the lifestyle changes, the patient could not expect significant improvement. We couldn’t have an unhealthy lifestyle and wait for a magical pill to erase and turn over at once, the years of unhealthy living. Therefore, regular exercise, stress relief, smoking cutoff, and a healthy diet are the cornerstone of a patient well being. Diet should be reduced in red and fat meat, processed food, and cholesterol, but reach in sea fish, olive oil, vegetables, and omega-3-acids. Some physicians recommend a glass of red wine a day, but excessive alcohol intake could severely affect your health.

MITRAL VALVE
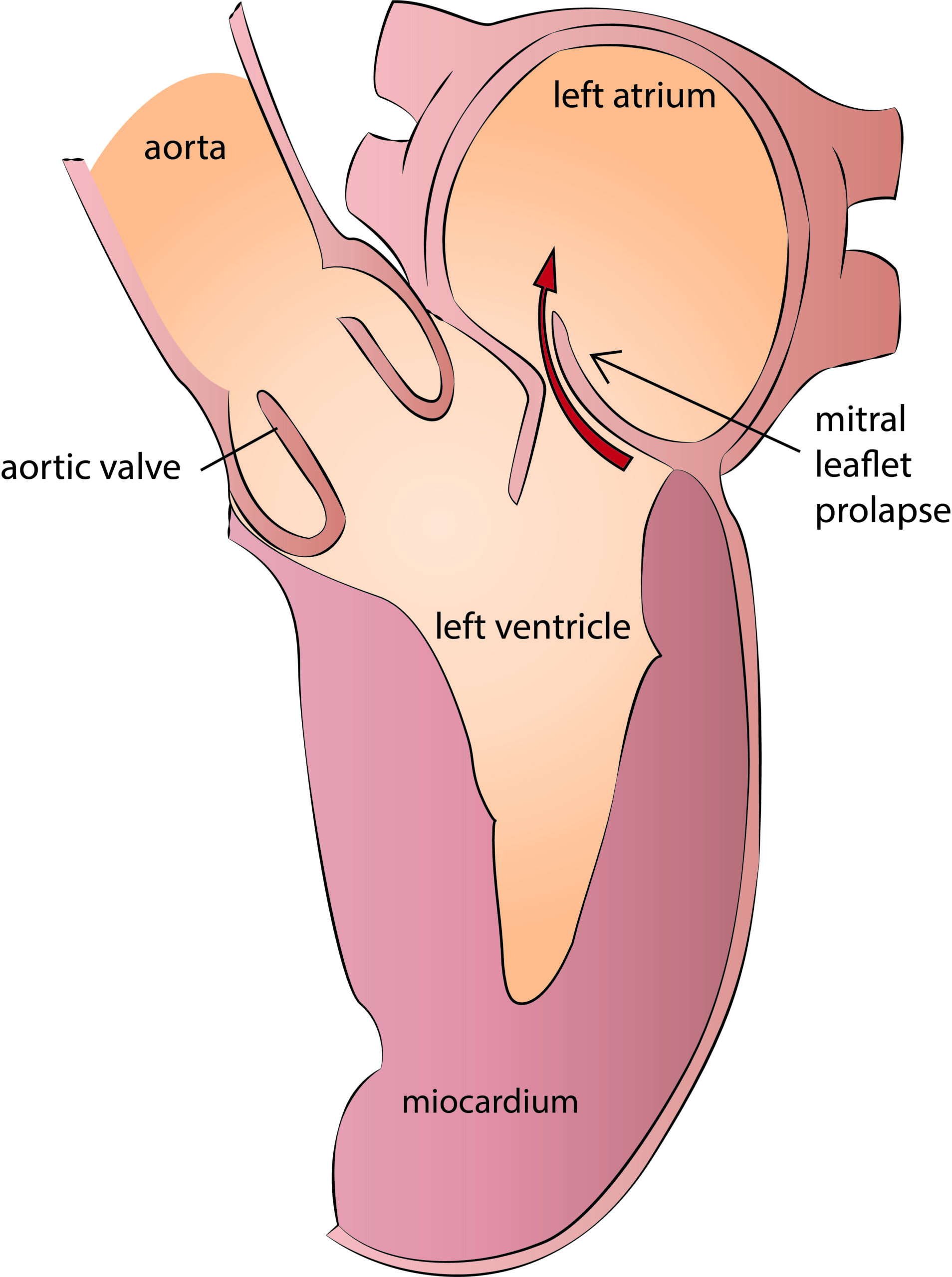
The Mitral valve is located between the left atrium and ventricle. Valve has two leaflets that are closed during the heart contraction providing the blood ejection in the aorta. During the heart relaxation, mitral leaflets open and let the blood to fill the left ventricle. That is how the mitral valve regulates the unidirectional blood flow through the left heart chambers. There two primary mitral valve dysfunctions. Leaflets open incompletely in the mitral valve stenosis, while in mitral insufficiency their closure is compromised.
Mitral valve stenosis used to be the leading cause of mitral disease in the pre-antibiotic era. Widespread antibiotic use, reduced the incidence of streptococcus bacteria infection and rheumatic fever, therefore. Unfortunately, rheumatic fever remains still a significant cause of mitral disease in undeveloped countries today.
Mitral valve insufficiency or regurgitation is the main form of mitral disease today. Due to degenerative disease, tendinous chordae gets elongated and eventually rupture, resulting in mitral valve prolapse. Prolapsed leaflet makes the valve incompetent, allowing the blood to regurgitate back into the left atrium. In cases of valve infection, or sometimes in acute myocardial infarction, the mitral valve prolapse and insufficiency have a sudden onset. Such a severe regurgitation is generally a medical emergency.
In chronic ischemic mitral valve insufficiency, the valve anatomy itself is preserved, but the coaptation is compromised by severe left ventricle dysfunction due to an old myocardial infarction.
Grace to the anatomy of the mitral valve, there is generally enough valve tissue to make the valve repair feasible. An experienced surgical team could repair more than 95 % of degenerative mitral valve disease. In ischemic or rheumatic disease, the mitral repair is still possible, but long term results are inferior comparing to degenerative mitral valve repair.
The echocardiography s a main diagnostic tool for the mitral valve disease. It could be done by a transthoracic probe applied on a chest wall or by a transesophageal probe from the esophagus, which provides a better view of mitral valve anatomy. The echocardiography grades the severity of the mitral insufficiency. Mitral regurgitation up to 2+ is considered hemodynamically insignificant and needs no further treatment appart of regular follow-up. Mitral insufficiency grade 3+ and 4 + is hemodynamically significant and has to be operated. In the mitral valve stenosis, the mean pressure gradient over 10 mmHg and valve orifice area inferior to 1 cm2 is considered significant and should generally be operated.
Sometimes it is not possible to repair the mitral valve, and we have to replace it.
The symptoms in chronic mitral insufficiency appear when the heart function starts to deteriorate. Patients could experience effort dyspnea or heart arrhythmias that are worsening according to myocardial dysfunction level. In advanced stages, shortness of bread is present even during daily physical activity or in rest. Mitral valve repair surgery should be therefore performed in early, asymptomatic stages of the disease to preserve heart function. Acute mitral regurgitation is poorly supported and is generally a surgical emergency.
AORTIC VALVE
The aortic valve is located between the left ventricle and the ascending aorta. The aortic valve has three tiny leaflets and opens during the ventricle contraction, allowing blood to ejection into the aorta. During the myocardial relaxation, valve closure prevents blood regurgitation back into the left ventricle. There are two main aortic valve dysfunctions, the aortic valve stenosis and insufficiency.
Aortic stenosis is a mainly degenerative disease that develops during the years in the same patients. Leaflets get rigid and less mobile and calcified eventually along with the aortic valve annulus. The heart compensates for increased pumping demands due to stenosis by myocardial hypertrophy. Patients are generally asymptomatic during this period. Symptoms onset is a sign that myocardium could not compensate the aortic stenosis anymore and are getting to fail.
Systolic heart murmur over the aortic valve, and the following symptoms are clear evidence of existing aortic stenosis:
- Sinkope – sudden loss of consciousness
- Chest angina – chest pain like in coronary disease
- Heart failure signs – shortness of breath during exercise or in rest
The symptom onset announces the terminal disease stage. Life expectancy with the emergence of syncope or chest angina is around 5 years, while those with heart failure signs have a life expectancy of 2 years. Therefore, it is a priority to diagnose and operate aortic stenosis while the heart function is still preserved. Aortic valve replacement is the treatment of choice in aortic valve stenosis.
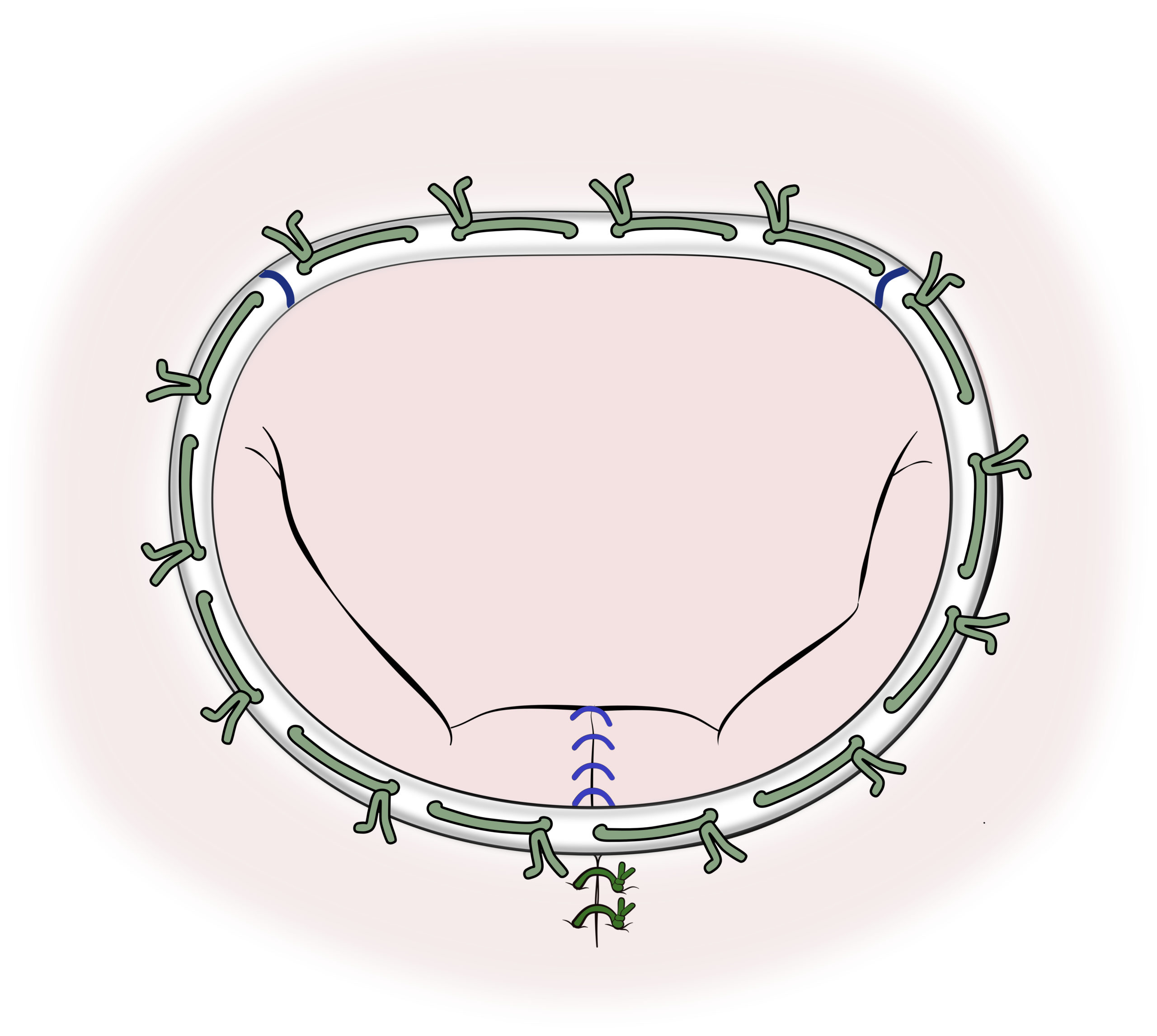
A small image demonstrates a widely opened aortic valve in systole. Thick and calcified leaflets have restricted motion and do not open completely.
Leaflet closure is compromised in the aortic valve insufficiency allowing the blood to regurgitate back into the left ventricle. Similar to other valve diseases, such a volume overload dilates the left ventricle that eventually fails. Patients better tolerate chronic aortic valve insufficiency compared to the aortic stenosis. Anyway, valve replacement or repair are treatments of choice.
Acute aortic insufficiency, along with a high temperature, is highly suspicious of bacterial endocarditis. This a severe, most frequently bacterial valve infection that requires immediate hospitalization, antibiotic treatment, and valve replacement surgery. If a new-onset aortic valve insufficiency is followed by a sharp, excruciating chest pain that spreads from chest to the back or legs, the patient is probably suffering from an acute aortic dissection. That is, of course, a surgical emergency that has to be operated almost immediately to prevent fatal aortic rupture.

Surgical treatment is a gold standard in aortic valve disease. Medication could reduce symptoms but without the surgery heart failure is inevitable. Either mechanical or biological prosthesis could replace the aortic valve. The mechanical prosthesis is durable but requires lifetime anticoagulation therapy. Tissue valves are made either of the bovine pericardium or from porcine valve tissue. They have limited durability, but need no lifetime anticoagulation and are implanted in older patients, generally those above 65 years.
AORTIC VALVE REPAIR
Aortic valve repair is by war the best solution in aortic valve disease. We are preserving the patient’s valve and make it fully functional, with almost no foreign material implanted. We repair mostly regurgitant aortic valves since stenosis is almost impossible to reconstruct.

TAVI PROCEDURA
TAVI. Transcatheter Aortic Valve Implantation is an interventional aortic valve replacement without the surgery. Biological or tissue prosthesis is implanted using a system of catheters placed through the femoral artery. Older and high-risk patients are the best candidates for TAVI.
AORTA
ANATOMY
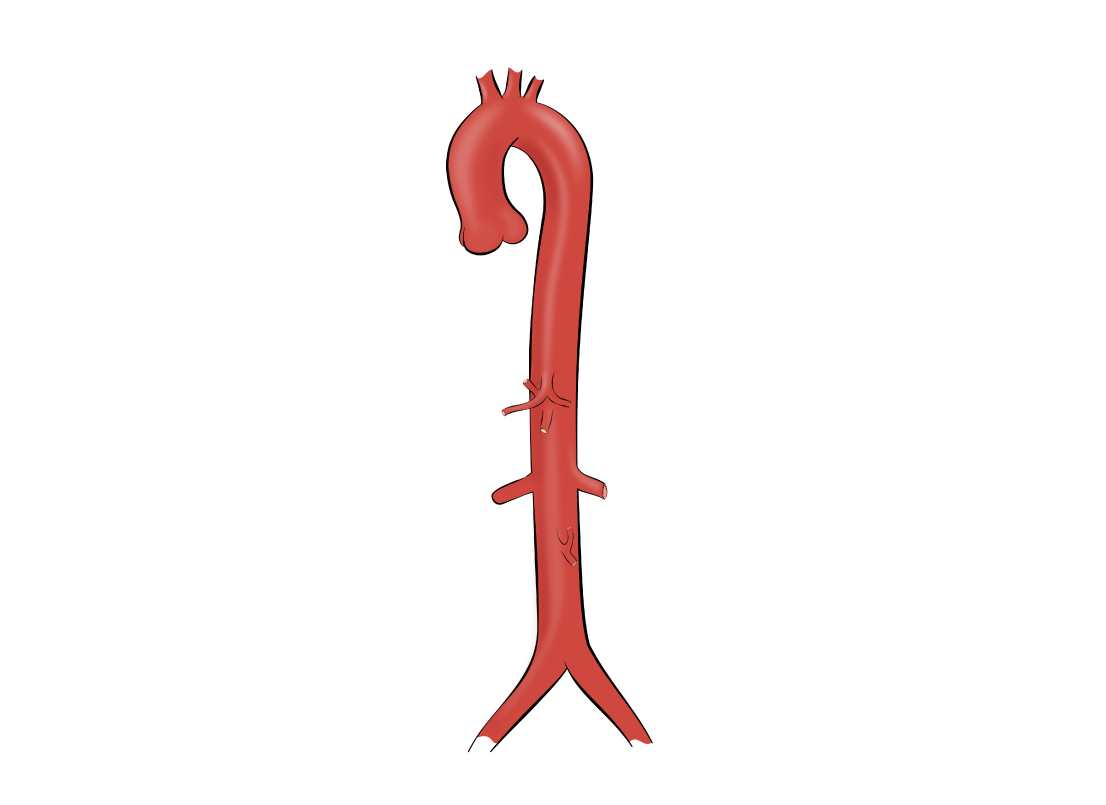
Aorta is the major and the biggest artery in the human body. Aorta emerges directly from the left ventricle and the aortic valve, and after that branches to deliver the blood to the brain and other organs. Aorta is exposed to high pressure and volume load during the left ventricle contraction and blood ejection. The thoracic aorta has three segments. The ascending aorta is the aortic portion that emerges directly from a heart. At the level of a collar bone, it continues as an aortic arch, and thereafter downward as descending aorta. Bellow, the diaphragm level aorta continues as an abdominal aorta. Coronary arteries are the first two branches of the ascending aorta, while the brain and arm vessels branch out from the aortic arch. Abdominal aorta branches perfuse abdominal organs and kidneys and terminate by iliac arteries that perfuse the legs.
AORTIC ANEURISM
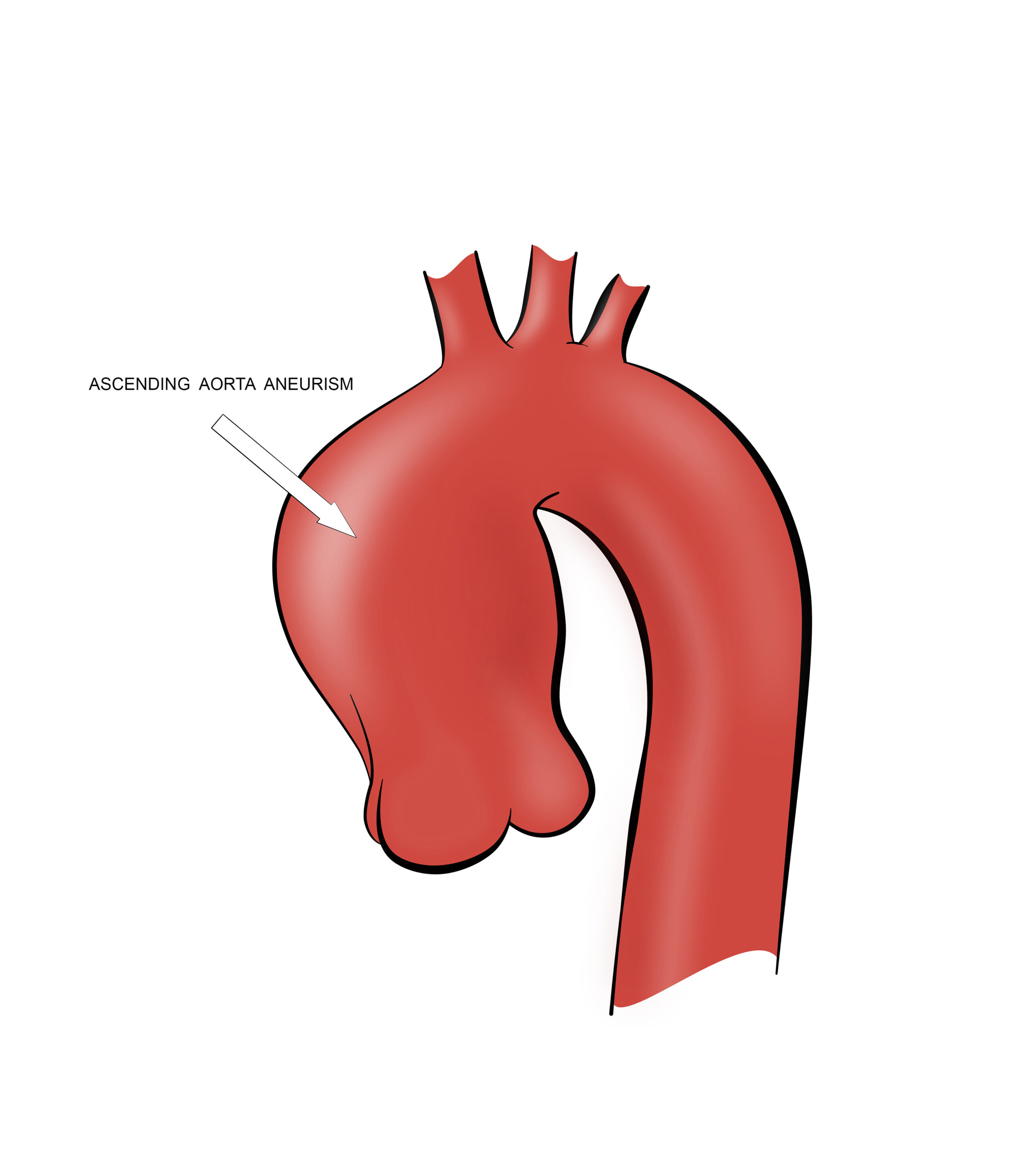
Aortic aneurism is a significant aortic dilatation. A healthy thoracic aorta diameter is up to 50 mm, and dilatation over 50 mm is considered an aneurism. Degeneration of the aortic wall tissue is the leading cause of the aneurism. That could be due to aging or to a congenital connective tissue disease, like in Marfan or Ehler-Danlos syndrome, for example. Aneurisms are rarely symptomatic, and therefore frequently discovered accidentally during some other chest diagnostic procedure. Generally, echocardiography and MSCT scans are the main diagnostic tools.
A sudden rise in blood pressure could result in aortic aneurism rupture. According to the Laplace law, the increased diameter increases the pressure on the vessel wall. Therefore, the probability of aneurism rupture rise with its width as well. Surgical treatment is indicated if aneurism diameter is above 55 mm, or even less if another cardiac surgery procedure is performed.
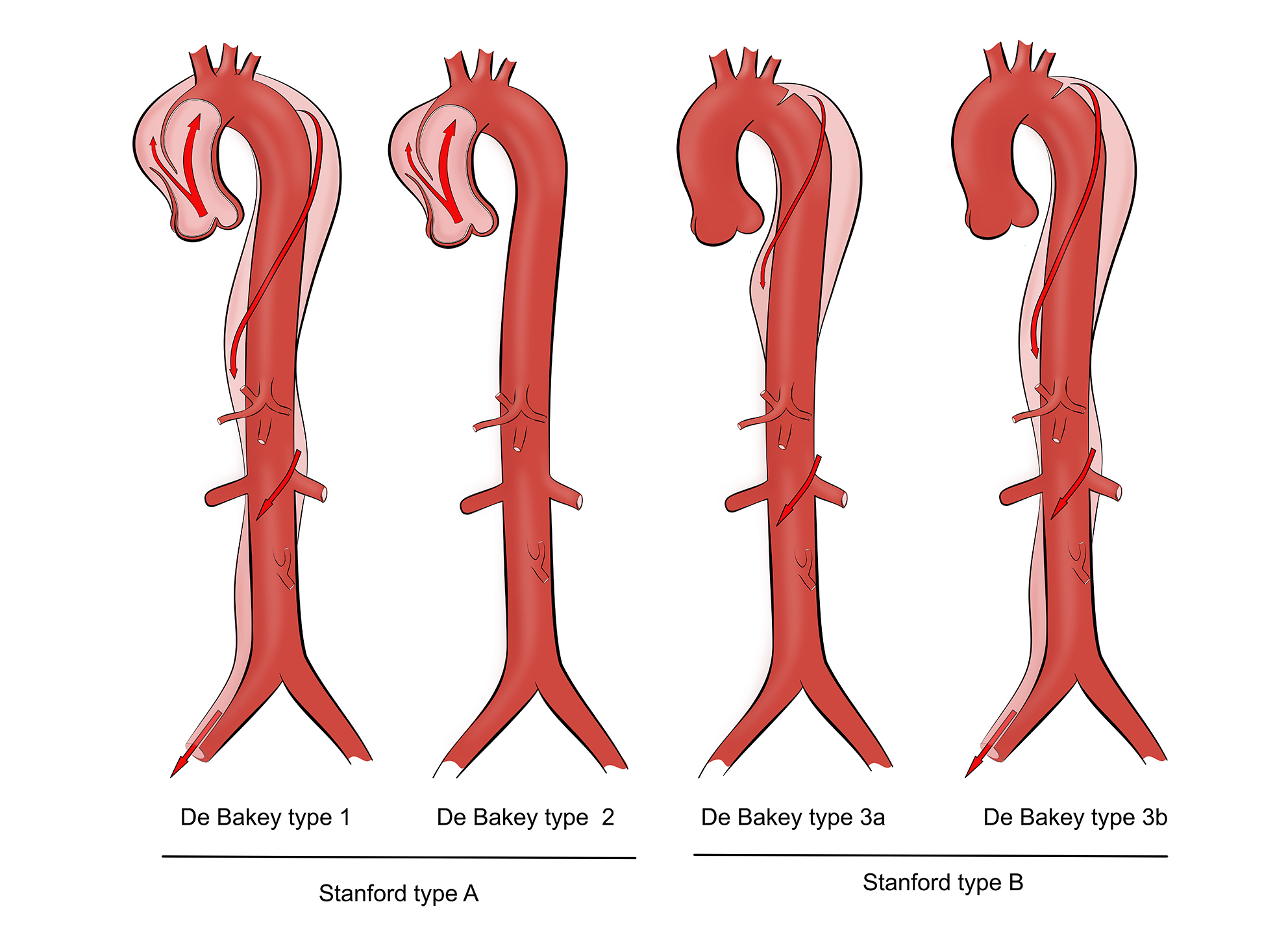
AORTIC DISSECTION
Aortic dissection is a surgical emergency that happens when a sudden rise in blood pressure tears up an aorta from inside. That is an entry point for blood flow to enter and dissect throughout the aortic wall. Dissection most frequently starts at the ascending aorta and spread out after that. Sharp, excruciating chest pain radiates interscapular or down the legs, is the main symptom of aortic dissection. Without the surgery, most patients will die due to aortic rupture.
CONGENITAL HEART DISEASE IN ADULTS
Urodjene srčane mane kod odraslih osoba su urodjeni defekti srčane anatomije koji nisu ometali normalan razvoj organizma do odraslog doba, tako da ranije ili nisu bili otkriveni ili još uvek nije bilo potrebe za njihovim lečenjam.

Following congenital heart diseases, do not affect growth and body development seriously and therefore, could be diagnosed in adults.
- Atrial septal defect (ASD) – The secundum type. That is a congenital defect of the interatrial septum that allows blood flow between the left and right atria. In the majority of adults, ASD is asymptomatic and found accidentally. Depending on the size, defect either affects heart function or allow eventually venous blood clots to pass and embolism the arteries. That is why we have to close them. Percutaneous closure devices are used to close moderate size defects with nice landing rim for the device. Surgical treatment is an option for the defect that is not suitable for percutaneous intervention.
- Atrial septal defect (ASD) with mitral leaflet cleft – the primum type. Interatrial defect in primum type ASD is positioned in lower septum along with anterior mitral cleft. Surgery is the only option for primum type ASD. The defect is closed by a bovine pericardial patch along with the mitral valve repair.
- Ventricular septal defect – VSD. Congenital VSD is rare in adults. It is located in the membranous interventricular septum and should be closed surgically or percutaneously.
- Persistent ductus arterious (PDA). Ductus arteriosus is a fetal communication between the pulmonary artery and the aorta that closes during childbirth. If still opened in adults, PDA raises the risk of bacterial valve infection, pulmonary hypertension, or heart failure and needs to be closed, therefore. It could be closed by surgery or percutaneously by specially designed coiling devices.
- Ebstein anomaly is a congenital malformation of a tricuspid valve in which their leaflets are adherent to the right ventricle or displaced down, reducing the size of the right ventricle and making right atrium very large. Tricuspid valve malfunction, along with altered right heart chamber anatomy, results in right heart failure and has to be operated.
- Aortic coarctation is congenital stenosis of a descending aorta. Patients suffer from upper body hypertension, the risk for coronary artery disease, valve infections, aortic aneurysms, and rupture or heart failure. Surgery is indicated when the pressure gradient over the coarctation is greater than 30 mmHg.
Ovo su samo najčešće mane kod odraslih koje se mogu uspešno lečiti hirurškim ili interventnim putem. Potrebno je znati da prisustvo većine urodjenih mana kod odraslih zahteva antibiotsku prevenciju bakterijkog endokarditisa (odlazak kod zubara i sl.) Za urodjene mane kod dece treba kontaktirati isključivo pedijatrijskog kardiologa i kardiohirurga.
HEART TUMORS
Around 75 % of heart tumors are benign, and approximately 50% of them are myxomas. Malignant tumors are rare and mostly secondary due to distant malignancy with heart metastasis.
Mixomas are the most common heart tumors. They are benign and could be present as an inherited disease in 5%, or as a sporadic form in 95% of cases. They are generally located and attached to a left atrium by a broad pedicle that allows them to float during the heart contractions. Mixomas are rarely symptomatic and therefore found accidentally during routine echocardiography check-up. Symptoms, if present, are caused by either embolization by tumor particles, or syncope due to valve orifice obstruction. Symptomatic myxomas are surgical emergency, while asymptomatic ones should be operated upon diagnosis to prevent future complications.
Fibroelastomas are small, frondlike tumors covered with tiny filaments that could detach and embolize elsewhere. They are generally located on heart valves that could be repared after tumor resection.